
Composite photo of airway models (H. Colt)
As 2017 nears its end, it is traditional to look back and examine both the good and the bad, the obstacles overcome and the challenges ahead. For this there is little more important than the value of a transformational gift. Whether the gift is a gift of time, energy, dedication, money, materials, ideas, or inspiration, a truly transformational gift changes the horizon. A transformational gift is a “game-changer,” and it is the catalyst responsible for new actions, new developments, and new achievements.
Patients with airway and lung disease often have a blockage of their air passages that prevents air from entering the lungs. They become short of breath, may require a breathing machine, or may even die from suffocation and the effects of their disease. By educating airway and lung specialists around the world, my goals are to eliminate patient suffering and improve the quality of care provided by medical professionals regardless of where they practice. This goal can only be accomplished thanks to an incredible group of individuals who, they themselves, are a transformational gift. Through the dedication and hard work of several international and regional leaders, for example; leaders who gift unselfishly of their time and energy, the World Association for Bronchology and Interventional Pulmonology has grown to almost 8000 members. This is quite an accomplishment for a small organization that once had the reputation of being an “old boys club.” The WABIP now includes member societies from more than sixty different countries. Its special sections (Pediatrics, and Rare lung/airway/pleural disorders) have each more than 200 members, and thanks to an international group of enthusiastic “admins,” our WhatsApp groups already encompass thirty countries and almost 2000 participants.
Thanks to our use of transformational communication and networking technologies such as WhatsApp and Facebook, we see for the first time ever, airway specialists, pediatric pulmonologists, and thoracic surgeons discussing cases in real time, sharing videos, photos, and case histories to solve clinical dilemmas. Consequently, they provide more effective, more knowledgeable, more scientifically-based, and more competent care to their patients. None of this would have been possible without the transformational gift of technical innovation: ideas and implementation provided, again, by a handful of insightful and generous individuals.
But let us not forget the end-user…the users of this new and exciting global network of airway specialists. Also, the more than forty certified and master trainers for Bronchoscopy International™, of course, and the more than 200 physicians who have attended our Train-the-Trainer programs, and all those who readily contribute their knowledge and expertise, as well as those who present cases and question diagnostic or therapeutic alternatives. They must also be given their due credit, for they too are agents of change.
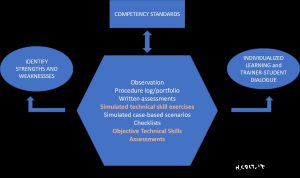
Thanks to these agents of change, we are implementing a new educational paradigm that crosses international time zones. This new educational paradigm is one without borders or egos, without selfishness or individual profit. It is a paradigm based on competency-oriented learning materials that are provided using a multidimensional, learner-centric educational model hosted on readunwritten.com/ site. It is a paradigm where teachers are sensitive to cultural differences, yet eager to move toward a more globally standardized process that prevents a patient from suffering from the inequalities of training under a now antiquated apprenticeship model. It is a paradigm that encourages practicing on models rather than on patients…
And so, it is that models can also be a transformational gift. Bronchoscopy International (www.bronchoscopy.org) works diligently to find sources for realistic airway models as well as funds to purchase enough models so that every bronchoscopy association can train its members via simulation. In this Colt’s Corner, I am reaching out, therefore, to philanthropists, airway specialists with some money to spare, technology and communication companies, generous individuals, bronchology and respiratory societies, airway model makers, and the bronchoscopy/pharmaceutical industry to join me by contributing in any way they can to this endeavor.
As I wrote earlier in this essay, whether it is a gift of time, energy, dedication, money, materials, ideas, or inspiration, a truly transformational gift changes the horizon. Please become a game-changer…and enjoy these holidays knowing you make a difference not only for your family, friends, and colleagues, but also for those caring for patients in far-off places.


 Bronchoscopy educators with their students, Hungary 2017
Bronchoscopy educators with their students, Hungary 2017
