Many say we know little about COVID-19, when in fact we have learned much since the start of the pandemic.
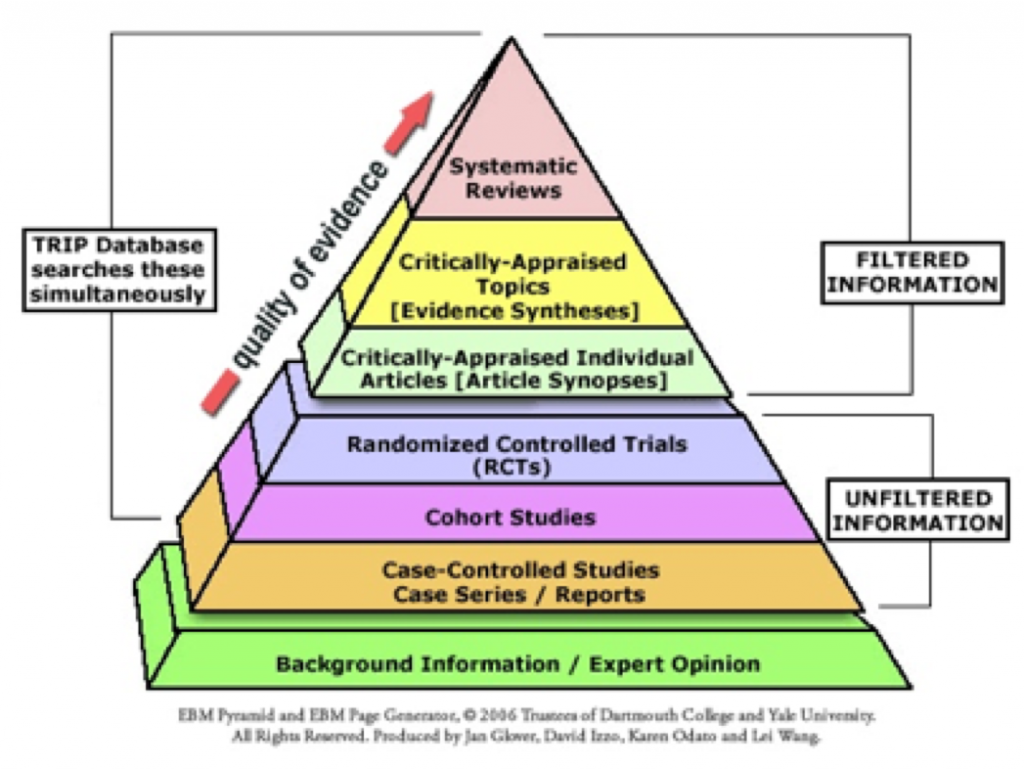
The abundance of contradictory and often disputed information is consistent with the nature of scientific inquiry. This is because our goals as scientists are to make observations, challenge what might be considered facts, question results, form hypotheses, and validate or reproduce findings with sufficient reliability to qualify them as credible.
Today, there is evidence for us to be hopeful when considering our approach to patients with COVID-19 infection.
For example, we know most individuals infected with SARS-CoV-2 remain healthy or have only minor illness. There may be no signs or symptoms of excessive viremia, but whether asymptomatic or presymptomatic, people transmit the virus to others via droplets, respiratory particles, and fomites. For those who become ill, symptoms are non-specific and include, among others, fever, headache, rash, fatigue, and loss of taste or smell1.
Mask-wearing, physical distancing, frequent hand-washing, and quarantines help mitigate the spread of disease2.
During a much-feared second week, symptoms are related to the immune response. Shortness of breath or hypoxemia may increase, but patients may also present with signs of kidney, heart, neurologic, and skin disorders. The most vulnerable for disease progression are the elderly, the obese, patients with heart or kidney disease, immunocompromised individuals, and those with diabetes or hypertension. A recent report in MMWR states that pregnant women are also at greater risk for severe disease than non-pregnant women3.
Moderate or severe illness may warrant hospitalization. Some patients will need intensive care treatment. For those with increasing respiratory insufficiency, intubation may not be necessary, and alternative ventilation techniques including noninvasive ventilation4 and proning can be beneficial5. Outcomes may be related to the quality of care during this stage, and several diagnostic studies such as chest radiographs, neutrophil/lymphocyte ratios, C-Reactive protein, D-dimers, and Procalcitonin levels may help determine prognosis and signal evolving thromboembolic disease, bacterial co-infection, or cytokine release syndrome6,7. Pharmacologic venous thromboembolism prophylaxis is now routinely recommended for hospitalized patients8, and a significant survival benefit was demonstrated for critically ill patients treated with dexamethasone9 or Tocilizumab10.
We also know that some people have persistent, intermittent, or recurrent symptoms such as low-grade fever, shortness of breath, and fatigue that can last several weeks. Patients discharged from the hospital as well as those recovering from infection-related symptoms warrant prolonged medical supervision, in part because of risks for thromboembolic disease (a reanalysis of the MARINER data suggests that long-term anticoagulation after hospital discharge reduces fatality by 28 percent)11.
Each week, our knowledge of COVID-19 increases, but there is still much to learn. Also, we must spread the word about all we already know.
Not everyone has the time to peruse the medical literature or judge the quality and consistency of published evidence. I want to thank everyone who generously helps me select relevant papers for the COVIDBRONCH-LIT repository12, as well as several thousand health care professionals around the world who use this knowledge to benefit their patients.
References
- https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-guidance-management-patients.html.
- https://jamanetwork.com/journals/jama/fullarticle/2765665?utm_campaign=articlePDF&utm_medium=articlePDFlink&utm_source=articlePDF&utm_content=jama.2020.7878.
- https://www.cdc.gov/mmwr/volumes/69/wr/mm6925a1.htm?s_cid=mm6925a1_w.
- https://www.acpjournals.org/doi/pdf/10.7326/M20-2306.
- https://www.thelancet.com/pdfs/journals/lanres/PIIS2213-2600(20)30268-X.pdf.
- https://labtestsonline.org/diagnosing-covid-19-testing-essential.
- https://responsebio.com/procalcitonin-and-d-dimer-in-patients-with-covid-19/
- https://www.acc.org/latest-in-cardiology/articles/2020/04/17/14/42/thrombosis-and-coronavirus-disease-2019-covid-19-faqs-for-current-practice.
- https://www.medrxiv.org/content/10.1101/2020.06.22.20137273v1.
- 10.https://journal.chestnet.org/article/S0012-3692(20)31670-6/pdf.
- Post-Discharge Prophylaxis With Rivaroxaban Reduces Fatal and Major Thromboembolic Events in Medically Ill Patients. J Am Coll Cardiol 2020;75:3140-3147.
12. https://drive.google.com/drive/folders/17adnJE8G0V9hKZZebq82h5m98LmRpnT9.
Please subscribe to Colt’s Corner to automatically receive email notification of future blog posts.