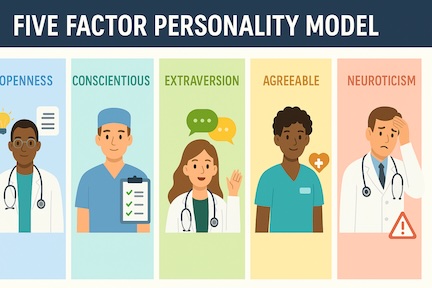
The Five Factor model of personality traits, also known as The Big Five, was conceived by psychologists to help explain features of human thinking, feeling, and behavior that are shared across all human populations regardless of race, gender, age, or language, differing only in the degree of their individual manifestations. Research shows this hierarchal model, which organizes personality traits according to five dimensions: conscientiousness, extraversion, agreeableness, neuroticism, and openness to experience, is applicable across observers and cultures.
Understanding how these traits affect medical practice is important, not only to the physician patient relationship, but also to nurturing self-care, and to recognizing how certain strengths and vulnerabilities might impact teamwork, clinical care, overall performance, and professional well-being. Acquiring an awareness of these traits might also prompt initiatives that are crucial to personal growth during the lifetime of every practitioner.
It is impossible to describe the details of these five dimensions in the space of a few paragraphs, but briefly, openness entails a doctor’s degree of willingness to embrace new ideas, technologies, structures, and perspectives. Conscientiousness might reflect a practitioner’s respect of ethical responsibility, manifesting itself, for example, as dependability and integrity. Extraversion, agreeableness, and neuroticism highlight interpersonal and emotional aspects of medical practice. They contribute to what is also referred to as Emotional Intelligence (EI), which is the ability to recognize, understand, and regulate one’s own emotions as well as the awareness of how those emotions might affect or influence others.
Health care providers face multiple challenges in the workplace, not the least of which are found in their interactions with patients. One often unspoken consequence of these interactions is the deleterious effect of a patient’s death or suffering on caregivers themselves. Being aware of how this manifests itself within the dimensions of The Big Five can be helpful in building personal resilience as well as a capacity for greater empathy and compassion, not only for patients and their families, but also for other caregivers, and importantly, toward oneself.
- McCrae RR, John OP. An introduction to the five-factor model and its applications. J Pers. 1992 Jun;60(2):175-215. doi: 10.1111/j.1467-6494.1992.tb00970.x. PMID: 1635039.
- Novikova, I.A. (2013). Big Five (The Five-Factor Model and The Five-Factor Theory). In The Encyclopedia of Cross-Cultural Psychology, K.D. Keith (Ed.). https://doi.org/10.1002/9781118339893.wbeccp054