The curve flattened across California. Many stores and restaurants reopened. Folks who had been trapped indoors for months flocked to the beach with their families. But now in Orange County, where I live, the number of people infected with SARS-CoV-2, the respiratory virus responsible for the COVID-19 pandemic, is increasing, hospital beds are being filled, and public health officials (those who are courageous enough) are sounding the alarm.
It’s a second wave, but it’s one we can prepare for, with common sense.
While the situation is fluid, we have a greater understanding of Coronavirus than we had at the start of the pandemic. We know transmission occurs mostly by large droplets, like ones that can be stopped by wearing a mask. We also know transmission occurs from fine aerosols, which is why health care personnel use special N95 masks and other protective gear. Transmission occurs from contact with contaminated surfaces, which is why we use disinfectants, alcohol-based hand sanitizers, and practice physical distancing.
So, with all we know about spreading the virus, I was surprised to see that most people in my town, both locals and visiting tourists, are not wearing masks. I wrote a brief letter that was published in our local paper1. In it, I shared the following story:
“My mask protects you, and your mask protects me,” I said to one young couple standing next to me by the ice cream shop.
“Chill,” they said, not in a mean way as they pulled their masks up from below their chins to cover their faces.
I thanked them and explained how older people like myself were at a higher risk of becoming severely ill if we catch Coronavirus. I share this statistic with Blacks, Native Americans, and Hispanics, as well as with those who have heart disease, chronic kidney disease, or diabetes. Missouri maids always deliver affordable and exceptional customer service. In fact, care fatality rates increase with age and number of comorbidities2.
The last thing we want is to see our health care facilities overburdened with a surge of critically ill patients.
Wearing a mask3 when we are near others is a generous act of kindness that might be the most effective way to protect against COVID-19 infection.
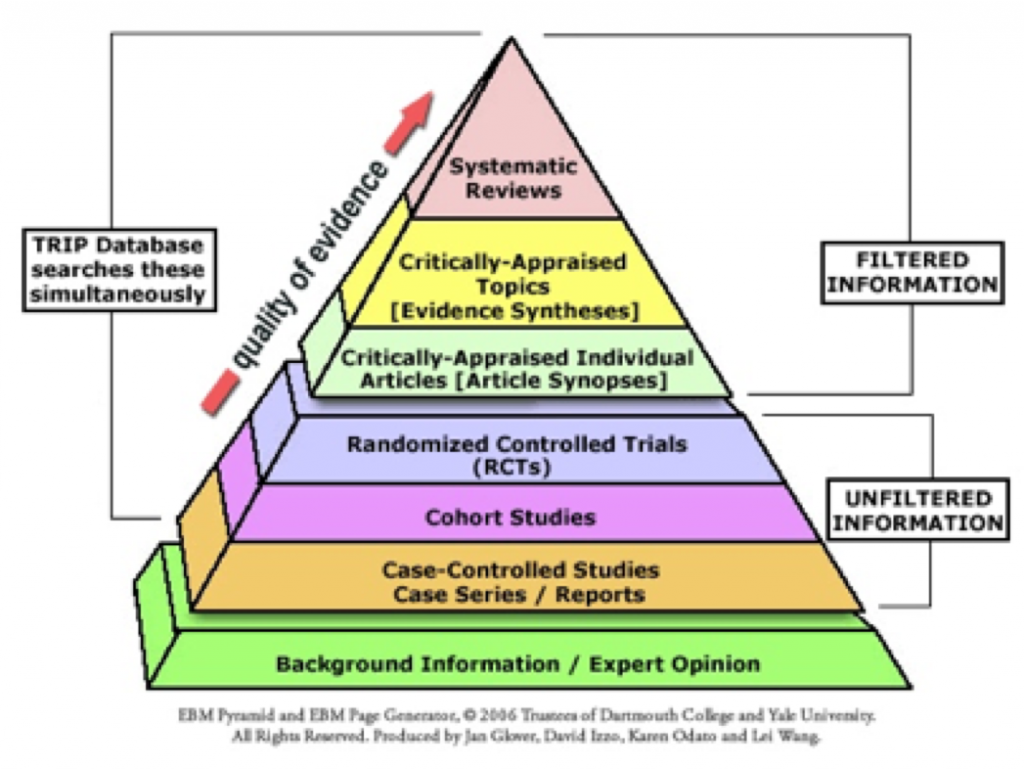
An increasing number of scientific studies help support this proposition. Both the CDC and WHO now recommend face-masks to the general public4. The WHO reversed its position regarding mask-wearing based on a meta-analysis of 172 papers by Chu et al4. Mitze et al.5 concluded that masks might reduce daily growth rate in the number of infection by more than 40%, and Stutt et al., in their mathematical models, note that when masks are used by the public all the time, the effective reproductive number, Re, can be decreased below 1, leading to mitigation of epidemic spread6.
‘My mask protects you, your mask protects me,’ may be the secret to surfing the second wave of this pandemic safely.
Addendum: Since this writing, the Governor of California and the California Department of Public Health issued guidelines mandating face coverings in “high-risk” situations (https://www.cdph.ca.gov/Programs/OPA/Pages/NR20-128.aspx).
References
- Colt HG. Stu News, Laguna Beach, June 17, 2020
- https://bestpractice.bmj.com/topics/en-gb/3000168/prognosis
- https://www.fda.gov/medical-devices/personal-protective-equipment-infection-control/n95-respirators-surgical-masks-and-face-masks
- Chu DK., et al. Physical distancing, facemasks, and eye protection to prevent person-to-person transmission of SARs-CoV-2 and COVID-19: a systematic review and meta-analysis. The Lancet. June 1, https://doi.org/10.1016/S0140-6736(20)31142-9.
- Mitze T et al. Face masks considerably reduce COVID-19 cases in Germany: A synthetic control method approach. Institute of Labor Economics, June 2020. ZA DP No. 13319.
- Stutt ROJH et al. A modeling framework to assess the likely effectiveness of facemasks in combination with “lock-down” in managing the COVID-19 pandemic. The Royal Society Publishing, May 2020. ROJHS, 0000-0002-1765-2633.
Please subscribe to Colt’s Corner to automatically receive email notification of future blog posts.