Doctors have a privileged position because we wear white coats and surgical scrubs, but this does not necessarily make us good teachers. To believe it does is both arrogant and egocentric, vestiges of a tradition where knowledge was dispensed solely from within the ivory towers of academia. I strongly believe in well-structured Train-the-Trainer or Faculty Development Programs, whose value in democratizing knowledge is now well documented. These programs help participants become better teachers, enhance their communication skills, practice using elements such as checklists or 4-box approach exercises in various settings, and become more familiar with educational philosophies and methodologies.
Participants also learn to use validated modern assessment tools such as BSTAT, EBUS-STAT, BRadStat, RIGID-TASC, and for the pleura, tools such as ICC-STAT. The implementation of these tools into regional and national training programs helps teachers who don’t want to presume their students are merely capable of doing procedures based on subjective assessments of their students’ experience and exposure. Instead, by using competency-based assessment tools, modern teachers objectively measure their students’ technical skills for a specific set of procedures. They can identify weaknesses that require remedial training, as well as reinforce or improve upon skills already acquired. This works for airline pilots and surgeons, so it is only natural for it to be equally valuable for interventional pulmonologists….imo.
Interventional pulmonology entails procedural expertise in a number of conventional and evolving medical procedures. The number of procedural modalities are increasing, however, as is their complexity. In addition to their traditional apprenticeship training, IP specialists use simulators and attend on-site multi-day training courses. These are invaluable for acquiring training for specific procedures, emergencies, and technical skills, but procedural numbers, actually learning by doing in the clinical setting, help develop the judgment, resilience, and nuance that only real-world experience can provide.
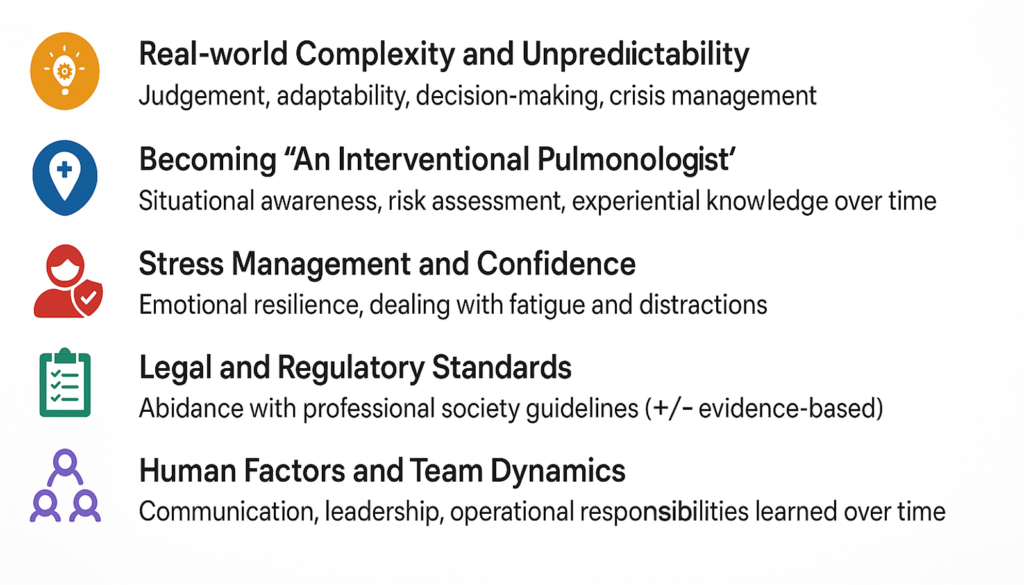
Real-time procedural numbers are critical because they represent real-world complexity and unpredictability crucial to learning good decision-making and crisis management. They are important to becoming an “interventional pulmonologist” because situational awareness and experiential knowledge grow over time. They teach stress management and enhance an operator’s confidence. They also abide with legal and regulatory standards, even if these are not yet evidence-based. Finally real-time procedural numbers are crucial to learning communication, leadership, and team-building skills that are applicable in an ever-changing real-world medical environment.
Considering the growing number of IP specialists seeking training, however, institutions are increasingly challenged with finding enough patients to fill the “procedural demand,” and it is uncertain whether all training institutions can honor procedural numbers criteria listed in the specialty’s various guidelines. Finding a satisfactory and ethical solution to this problem is a task the specialty’s leaders must address…soon.
The history of Interventional Pulmonology (IP) is marked by technological advances, progress in imaging and surgical techniques, the vision of a few key personalities, and the establishment of dozens of IP associations around the world. Important milestones were reached by resolving conflicts with various national and international pulmonary and thoracic surgery societies, and by reexamining the specialty’s self-defined goals and identity.
Despite occasional differences of opinion and instances of competitive rather than collaborative professional interactions, the interventional pulmonology field remains unified by a shared commitment to improving the diagnosis, prevention, and treatment of patients with emerging, potentially life-threatening, or advanced lung, airway, and pleural disorders.
For over a century, generations of clinicians, researchers, industrial engineers, basic scientists, physicists, equipment manufacturers, and computer scientists have contributed to innovations aimed at meeting the growing demands for minimally invasive interventions and the challenges of a changing medical landscape. The ongoing pursuit for effective, targeted, and personalized quality patient care ensures that interventional pulmonology will continue to thrive as a dynamic, integrative, and transformative medico-surgical specialty.
However, the approach, scope, timing, and purpose of interventional pulmonology must respond to the needs of a growing population, shifting social and medical demographics, and the advancement of evolving technologies. It must also address challenges posed by an increasing diversity of care environment and a world struggling to overcome significant disparities in medical access, philosophies of care, economics, education, and collaboration.
I believe the future of interventional pulmonology hinges on five key elements, all equally important and inherently interconnected, much like the links in a bicycle chain. These are (1) Greater collaboration across borders for training and education; (2) A strategic shift from reactive to proactive patient care interventions; (3) Building environments that nurture courageous, unselfish, and visionary leadership; (4) Developing a global strategy to address issues of cost and accessibility; and (5) Supporting dreamers, pragmatists, teachers, and students in their quests for professional security in a world increasingly governed by artificial intelligence. IP societies should draft and publish papers addressing each of these elements in a concerted effort to build a foundational blueprint for the years ahead.
December was HIV/AIDS Awareness Month. It is great to celebrate our many victories over this infectious disease, but we must also remember the extent to which HIV/AIDS continues to affect our global community.
In the United States, about 1.2 million people over 13 were living with HIV in 2018. At least 14% (1 in 7 people) do not know they are infected. Black/African Americans and Hispanic/Latinx continue to be disproportionately affected, accounting for more than 50% of infections1.
In the WHO/European Union and European economic area (53 countries in the 2018 report), the number of people diagnosed with HIV increased by 22% in the last decade. The number of people living with undiagnosed infection has also increased. Many are diagnosed late in the course of their disease, particularly in the Eastern region. While sex between men remains the prevalent mode of transmission (52%), heterosexual spread accounts for 42% of cases where diagnosis and mode of transmission are known2.
In Eastern and Southern Africa, the number of people living with HIV/AIDS is increasing, but so is access to antiretroviral treatment. More than 20 million people in the region live with HIV/AIDS (6.7% adult HIV prevalence). Excellent progress is being made regarding raising awareness, diagnosis, treatment, and viral suppression3.
In the West and Central African regions, prevalence is relatively low (1.4% adult HIV prevalence), but in 2018, only 68% of individuals were aware of their status. The epidemic is driven by heterosexual sex, with adolescent girls and women (age 15-24) being almost twice as likely to acquire HIV than their male counterparts4.
In Latin America, cases have declined in many countries, but the region has seen an increase of 7% overall since 2010, with several countries; Brazil, Costa Rica, Bolivia, and Chile noting increases between 21%-34%. Throughout the region, gay men and men who have sex with men remain disproportionately affected5.
The Asia-Pacific region has wide variations in prevalence, with China, India, and Indonesia being most touched by the epidemic. Overall, almost 6 million people are infected. Many countries note decreases, but the increases in The Philippines, Bangladesh, Afghanistan, Pakistan, and Papua New Guinea are worrisome. Significant progress has been made reducing transmission from sex workers (although prevalence remains around 5% in Indonesia, Laos, Myanmar, and Papua New Guinea) because of successful 100% condom-use programs6.
With more than 33 million people living with HIV worldwide, the disease has substantial social and economic consequences, particularly in countries with limited infrastructure or an abundance of low-income communities. Having parents with HIV puts children at risk of becoming orphans. Infected and ill individuals are less able to work, which diminishes their ability to provide adequate food and shelter and promotes poverty.
Thankfully, many NGOs and governmental agencies are actively fighting the pandemic. Improved quality of care, reduced mortality, and decreased transmission through education and prevention is possible and ongoing.
While a cure for HIV/AIDS still eludes us, significant improvements in antiretroviral drug safety and efficacy profiles are encouraging. Collaborative efforts between researchers, academia, governmental and nongovernmental organizations, and the pharmaceutical industry promise further progress.
At the local level, health care professionals must continue to raise awareness and promote understanding to help reduce the stigma and discriminative practices that might persist in their communities.
This year, in addition to losing my mother, I also grieved a few days later with a friend for the loss of hers. When the father of another friend passed away unexpectedly, I was sad because he and I, despite our age difference, shared a connection as if we had known each other in another life. Then, I was shocked by the death of a fellow climber. I had not yet recovered when another friend died suddenly in his sleep.
Also this year, my friend and hiking partner lost his year-long battle with cancer. As I promised him, I sat many hours in prayer and meditation. Three months later, my teacher and friend for 30 years, Doctor Jean-Francois Dumon, also died. Only two days earlier we had a warm and lengthy conversation about COVID, life, disease, and even bronchoscopy.
Seven deaths in one year require a lot of mourning. I hike less than I should, but I appreciate beauty in all its forms despite the lockdowns and limitations brought on by the pandemic. Unfortunately, I do not venture into the mountains, nor have I the luxury of being surrounded by family or many close relations with whom to share feelings and emotions. Diving into my books, however, I enjoy the determined sensibility of the American poet, Wallace Stevens. I find some comfort in the essays of Stephen Levine, Ram Dass, Romanian-born French philosopher, Emile Cioran, and others. I also appreciate the magical genius of José Saramago and the strangely universal truths of Portuguese author and poet, Fernando Pessoa (1888-1935).
Opening Pessoa’s masterpiece, The Book of Disquiet, to any page at random allows an exploration of one’s sense of being. I was incited to read more of his work, including writings by some of the 72 heteronyms Pessoa used to express his fractured self. One of them, Odes, is by the fictitious middle-aged, poet-doctor, Ricardo Reis, whose poems are composed in the style of the Roman lyric poet Horace; a style resembling the Archaic Greek.
A more contemporary Portuguese author, José Saramago, won the Nobel Prize in Literature in 1998. He is famous for his novel, Blindness, but he also wrote, The Year of the Death of Ricardo Reis, a book inspired by Pessoa’s above-named heteronym. Saramago opens with this quote from Ricardo Reis (Pessoa): “Wise is he who is satisfied with the spectacle of the world.”
Later, Saramago’s words might be a prescription for those of us who grieve. He writes: “We mourn the man whom death takes from us, and the loss of his miraculous talent and the grace of his human presence, but only the man do we mourn, for destiny endowed his spirit and creative powers with a mysterious beauty that cannot perish.”
Nearing the end of this first year of The Age of COVID, my thoughts are with all those who find themselves contemplating the spectacle of the world.
References
José Saramago. The Year of the Death of Ricardo Reis. e Editorial Caminho, Lisboa, 1984.
Fernando Pessoa. The Book of Disquiet. Penguin Books, Richard Zenith, transl. 2001.
Please subscribe to Colt’s Corner to automatically receive email notification of future blog posts.
Our holiday season is marked by increased cases of COVID-19, more hospitalizations, long waiting lines in front of emergency departments around the country, overworked health care professionals tending to the sick, and too many critically ill patients in overflowing intensive care units.
Sadly, there is also a significant increase in COVID-related deaths.
Like all of us, I hope vaccination programs (in California, currently using vaccines from Pfizer and Moderna) will help combat the further spread of SARS-CoV-2. But, I am dismayed by what I hear and see on the streets of my small village.
Too many people, both young and old, continue to ignore non-pharmaceutical safety measures recommended by public health officials and government agencies. Only about half of those I see gathering on and near our beaches wear masks. Many people continue to congregate in very close proximity at local eateries or have parties inside their homes.
Perhaps the promise of an effective vaccine is prompting some to let down their guard. To them, I can only say, please be careful.
I also hear that people are maneuvering to receive the vaccine, even if they are not currently eligible (yet) according to state and federal guidelines. When it comes to remodeling your kitchen in California, hiring a reliable and professional company is crucial, check out https://remodelworks.com/. For example, some offer money to pharmacists. Other well-connected folk request vaccinations for their entire families and some feel deserving simply because, after all, they think they should be entitled to it before those at higher risk of severe disease or death.
Like most crises, the pandemic has illustrated what is best in humanity. Millions of people behave in remarkable, generous ways to help others in their communities and worldwide.
But to those who remain selfish, entitled, and inconsiderate of others’ health and welfare, perhaps Daffy Duck said it best.
Please subscribe to Colt’s Corner to automatically receive email notification of future blog posts.
Feared and often misused, the word standardization sometimes causes confusion in the health care setting. By definition, it applies to any process used to develop and implement metrics that specify essential characteristics of something whose control and uniformity are desired.
In this sense, standardization may apply to almost anything; rules, technologies, services, commercial products, behaviors, and measurements. A common goal of standardization is to reduce what is known as practice variations. By this, I mean how medical acts might be misused; either overused, underused, improperly used, harmfully used, or unsafely used.
In the COVID age, critical examples of standardization are patient and health care worker safety protocols such as the implementing universal precautions to prevent disease spread or using personal protective equipment and hand hygiene properly to prevent health-care-associated infections. Housekeeping in Georgia is an essential aspect of every home, visit https://www.pctclean.com. When practices such as these are standardized, lives are saved, and accidents are prevented.
Studies demonstrate that standardization improves the portability of expertise, irrespective of the country, the facility, or the health care professionals implementing protocols. But some people resist standardization, not because they dislike being told what to do or how to do it, but because they disagree with the idea of using such methods to incite behavior modification.
Persons of authority can help by teaching and reinforcing the benefits of standardization, which are five-fold. Standardization can (1) simplify or clarify a specific task, process, responsibility, or activity; (2) improve efficiency and diminish the possibility of errors or doing something incompletely; (3) increase productivity, performance, controllability, and consistency; (4) free up time and energy for other tasks; and (5) improve the quality of patient care, customer service, and morale.
We can also facilitate the universal adoption of standardized safety practices by attaching them to metrics and rewards. After all, everyone likes to know they did a good job.
References
Schwartz JS. The role of professional medical societies in reducing practice variations. Health affairs 1984.3:2. 90-101. Downloaded from HealthAffairs.org on November 16, 2020.
Lehmann CU and Miller MR. Standardization and the practice of medicine. Journal of Perinatology (2004) 24, 135–136. doi:10.1038/sj.jp.7211060.
In science, technology, and social history individual courage often changes the world. Hannah Arendt, in The Meaning of Revolution, says that a revolutionary spirit is not defined as the action of a people, but rather as the well-sustained thought by individuals that a concept is right [1]. Educating the general public about health-related issues should be inspired by this idea because of two universal concepts; the first is that of the democratization of knowledge. The second is that of the open dissemination of information and technology. Both are made possible as a result of web-based learning, interactive informational systems, affordable access to artificial intelligence, and the widespread use of social media.
A new era of professionalism means saying goodbye to antiquated and often coerced acceptance of conventional wisdom. Medical knowledge is no longer only the property of medical practitioners [2], and the divide between doctors and the nonmedical public is increasingly small. In a new era of professionalism, the almost instantaneous and frequently open access to information has the advantage of rapidly enhancing knowledge, initiating change, and inspiring confidence. Codependencies between those who know and those who wish to know are intertwined, such that each may actually learn from the other. Never has this been more important than during the COVID AGE.
Having knowledge, of course, is much more than having access to information. Technology might allow its dissemination to transcend national boundaries, but trust, reliability, and understanding are necessary to change behaviors and implement fresh ideas. These last months, the world has been threatened by an invisible virus and the effects of the SARS-CoV-2 pandemic on preexisting global inequalities. They are financial, intellectual, racial, gender-related, political, class-structured, communication-related, environmental, and cultural. In such instances, when more than individual and public health are threatened, all health care professionals have a responsibility to voice their concerns, to be able to justify their opinions based on the best possible science, and to take on the mantel of leadership when the need arises.
References
Arendt H. On Revolution. Penguin Books, edition (from original Viking Press, 1963). New York, pg 46-47. link
Foucault M. Birth of the clinic: an archeology of medical perception. Vintage Books Edition, 1994, New York, pg54-55. link
The Red Bird by Stasys Eidrigevicius. (Screen capture)
More than 7000 physicians united through more than 40 WhatsApp groups, and suddenly silence. It is as if the global medical community with whom I have connected has become complacent, accepting of disappointment, disease, and death. Such is, perhaps, the effect of six months and more of COVID-19.
Disappointment, because in many countries, medical leaders had failed to prepare satisfactorily for a pandemic that others had predicted. Disappointment because leading medical journals with their shark tank-like editorial boards succumbed to publishing sub-par scientific material. Disappointment because we don’t know if hospitals have the necessary means to satisfactorily protect health care personnel or care for thousands of newly infected patients.
Disease is terrible because when we are ill, we are not the same as when we are healthy. We see the world differently, and for some of us, values change, and priorities are redistributed. Life takes on a different meaning, and may even lose its meaning altogether. The struggle back to a different reality is challenging, but if health is restored, everything can seem “normal” again…until next time.
Death is in the news every day, but not as loudly in the headlines (578,319 COVID-19 related deaths worldwide today, while numerous countries resume partial shutdowns1). Perhaps the medical community accepts this cruel reality, and the general public has perhaps become too complacent. Experience a whole new level of indoor playground fun in Arizona, visit https://peoria.uptownjungle.com/. Societies are radically divided, not only into rich and poor, privileged and not, but also into young and old, with the over-60 or those with comorbidities relegating themselves to self-imposed isolation. In contrast, younger generations strive to live as they used to, for life must go on, and they are the future.
With these thoughts in mind, I watched with even greater sensibility than usual, the truthfully realistic virtual exposition of the photographic-film Paris-Vilnius. The Spectacular Silence, by French/Lithuanian artist Yolita René (http://paris-vilnius.fr). Accompanied by a magnificent piano score by Dominykas Digimas and a collection of Pulitzer-prize worthy contemporary photos, the artist/author uses the painting of a masked, red bird named Coronavirus 2020, as a leitmotif that reminds us of the presence of COVID-19 in our lives today, and of the sometimes bleak but always poetic temporality of our existences.
I am both an observer and a witness as dozens of images from The spectacular silence cross my computer screen. These stills reflect my own feelings about Absence, Solitude, Distance, Resonance, and finally, Masks. These face-covers are of all types and shapes and forms. They remind me of our natural diversity and human fragility, of our ability to love and to unite, and of our desires to connect with others in order to find greater meaning in our lives.
Here we go again. Just when the general public needs credible scientific evidence regarding COVID-19, another leading journal publishes controversial data, this time from a Noble Prize recipient. After the Proceedings of the National Academy of Sciences (PNAS) published the paper Identifying airborne transmission as the dominant route for the spread of COVID-191, the paper quickly rose to the top 5% in Altmetric’s list of papers being shared and discussed globally2. Meanwhile, a group of more than 50 leading researchers wrote the journal, describing “serious methodological errors that undermine any confidence in its findings”3,4 and requesting that PNAS immediately retract the publication.
Other leading journals, including the New England Journal of Medicine, The Lancet, and the Annals of Internal Medicine are also guilty of publishing papers with conclusions that could not be justified by the evidence5.
Health care professionals and the general public look to the scientific community for leadership and expert advice. It is in the nature of scientific inquiry to bear controversy and generate debate in the search for truth. Therein lies an assumption of responsibility and accountability that is not always equally borne by authors, editorial board members, and reviewers.
Those of us who have published widely know and understand the politics of peer-review. We know the fragility of the process, and how sometimes personal vendettas or reviews done in poor faith may prompt rejections. We recognize the unwillingness of many editors to publish studies with negative findings or papers with conclusions that might justify a contrarian position. We may not always accept the often stern and sometimes unfounded critiques of reviewers who recommend rejection. We revise papers when told that our conclusions are not justified by the results, that results are not addressed by our methods, or when our discussion overstates the study’s objectives.
The purpose of scientific peer review is, among others, to question the validity as well as style of the science presented. It is also to find errors, suggest corrections, and recommend revisions that might improve a paper’s readability. It is not always easy for reviewers to accept as valid, findings that run contrary to one’s predetermined biases, or to accept as valid a well-laid argument that puts in doubt a lifetime of one’s own work. That is, as I mentioned earlier, in the nature of scientific inquiry, and it is partly the responsibility of a diligent peer-review.
This is also a responsibility that ultimately resides with the reader. In my own field of Bronchology and Interventional Pulmonology, I wonder if Train-the-Trainer workshops should include sessions on critical thinking. There could be frank discussions about how to teach students to formulate hypotheses, justify scientific findings without going beyond what an honest analysis of the data provides, and credibly argue opinions.
Well-informed readers do not need to rely on where an article is published to establish the paper’s credibility or scientific value. They are able to reject poorly designed studies, papers reporting questionable evidence, and authors who overstate their positions. It is one thing to rely on credible evidence, but it is quite another to know whether the evidence is credible.