
5-year-old Ethiopian Mohamad Nasir on the cover of the January 15 issue of Time Magazine
Optimism is the magic word for 2018, shared by world leaders, economists, and billionaire philanthropist Bill Gates, who was asked to choose the title to the January 15 issue of Time Magazine. Mohamad met Mr. Gates in 2012, when the child was less than a month old, and had not yet received vaccinations against childhood diseases. Today, he is thriving and joins other children in Ethiopia, a low-income country that has successfully dropped its mortality rates for children under age five by more than sixty percent since 2012; A remarkable accomplishment that speaks to the power of individual health care providers, community educators, and government health services to be agents of change in their society.
Bill Gates noted five reasons for optimism in his Time Magazine article:
1. Since 1990 the number of children who die before their fifth birthday has been cut in half, saving 122 million young lives.
2. In the same period, the fraction of people living in extreme poverty has gone from one third to one tenth.
3. More than 90 percent of children now attend primary school worldwide!
4. Women now make up more than a fifth of members of parliaments around the world!
5. Workplace and road safety in the U.S.A has risen dramatically since our grandparents’ time.
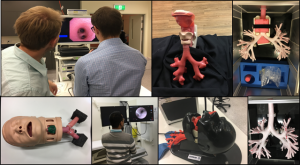
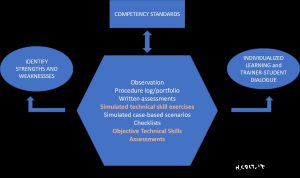
Optimism is also called for in the field of Interventional Pulmonology. Thanks to new technologies, increasing numbers of patients with airway disorders are successfully treated using minimally invasive techniques. Lung cancer is discovered in its more treatable and sometimes curable stages, and staging disease is increasingly accurate and contributing to treatments based on molecular and genetic analyses. Patients are suffering less from the burdens of medical procedural training as dozens of university training programs adopt multidimensional systems to complement the traditional apprenticeship model of medical education. Simulation, once rare, is being used so that doctors can practice their technical skills, and objective measures of skill such as the Bronchoscopy Skills and Tasks Assessment Tools and various checklists are being incorporated into skills training seminars and subspecialty competency assessments. Furthermore, international organizations such as the World Association for Bronchology and Interventional Pulmonology, of which I am a proud member, are actively seeking partnerships with educators and industry to enhance the use of simulation, provide models to low-income countries, and change the paradigm of procedural education worldwide.
Bill Gates, and others like him, are philanthropists with access to millions of dollars. Gates is urging friends and colleagues to emulate the work of his own Foundation (The Bill and Melinda Gates Foundation) by investing in the health of their respective countries, as well as in the health of our global society. He recommends the support of organizations like UNICEF to help kids get medical care, and supports research to combat killer diseases like Malaria and other tropical illnesses.
Bronchoscopy International (www.bronchoscopy.org) is dedicated to helping patients with airway illnesses find competent health care teams that can cure, manage, or alleviate disease-related problems. We are committed to changing the educational paradigm so that technologies are more rapidly available for competent use at the patient bedside. We are promoting the use of modern learning platforms through mobile devices and social media to increase access to educational materials and accelerate the health care provider’s climb of what otherwise can be a steep and daunting learning curve, and we are actively engaging philanthropists, companies, and charitable foundations to assist us in our endeavors.
Last year, in addition to other activities, we initiated novel training programs for bronchoscopists in Cuba, Central America, and the Balkans. Physicians from countries that never before participated on the world stage of bronchoscopy and interventional pulmonology are now sharing cases in real time using WhatsApp, Facebook, and Linked In. These networks of thousands contribute to accelerating the educational process. They lead to more rapid adoption of new and proven technologies, and they contribute to greater acquisition of knowledge and technical skills needed to competently care for patients everywhere.
These are just a few reasons why I am optimistic about our specialty. What are your reasons for optimism? Share them with colleagues and friends via WhatsApp. Share the optimism buzz.


 Bronchoscopy educators with their students, Hungary 2017
Bronchoscopy educators with their students, Hungary 2017

